

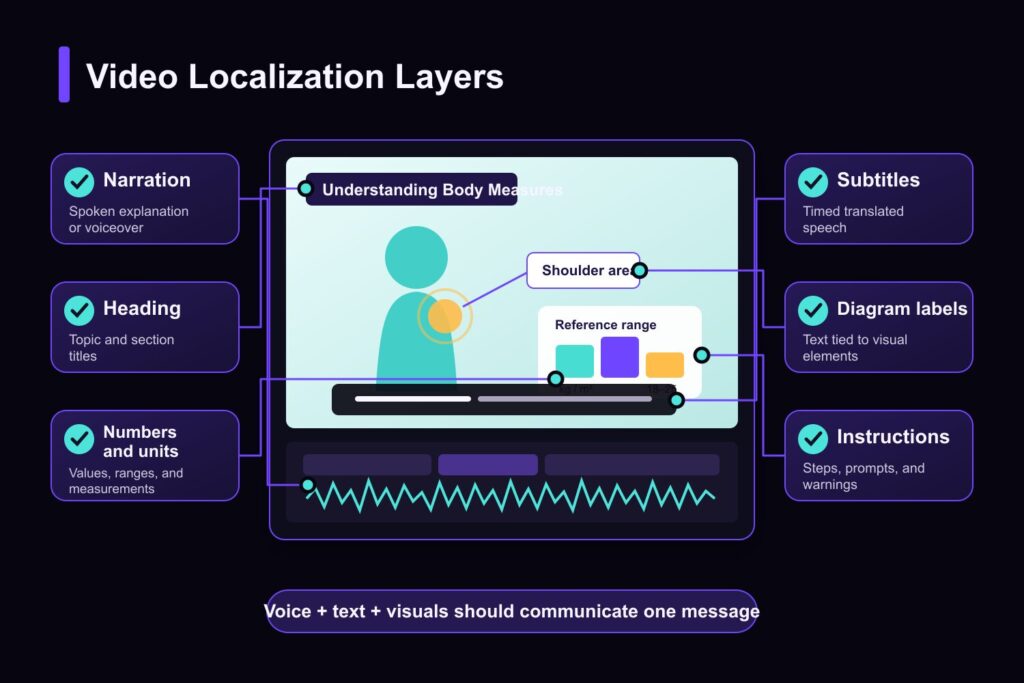
Patient education videos often carry meaning through more than narration. A video about body measurements may show values and category labels. A nutrition lesson may use food charts and portion graphics. An anatomy explainer may rely on arrows, body-part labels, or highlighted regions. If a multilingual version changes the voice and subtitles but leaves those elements in the original language, the viewer receives only part of the translated message.
This is not a hypothetical edge case. Recent video-localization activity reviewed for this content plan included BMI classification, nutrition and weight-management lessons, body-area explanations, health-related courses, and other instructional material built around visible text. The samples do not reveal every uploader’s role or organization, and they do not all qualify as patient education in the narrow clinical sense. They do reveal a consistent production requirement: healthcare educators, health-content teams, and medical or wellness education providers need to localize what viewers hear, read, and follow on screen.
A reliable workflow therefore treats the video as one connected information system. Narration, captions, diagrams, labels, numbers, and instructions should be translated in context and reviewed together.

What Is Patient Education Video Localization?
Patient education video localization is the process of adapting an existing health or patient-facing video for people who use another language. It can include translated narration, subtitles, Text auf dem Bildschirm, graphics, terminology, timing, and layout, followed by linguistic, subject-matter, and visual review.
Translation asks what the source says. Localization also asks who the target viewer is, which language variant they use, how much space the translated text requires, and whether the complete scene still communicates the approved meaning. That distinction matters in health education because the spoken explanation and visual layer often work as a pair.
The goal is not to rewrite medical guidance or make a translated video sound more authoritative than its source. It is to preserve the purpose, meaning, and usable structure of an approved source video for another audience.
Why Health Education Videos Need More Than Direct Translation
The World Health Organization defines health literacy around people’s ability to access, understand, appraise, and use health information. It also places responsibility on information providers to make trustworthy information understandable and actionable. Successful localization, then, is not measured only by whether every source sentence has a target-language equivalent. The complete material still has to work as communication.
Patient-facing language is not specialist language
Medical and public-health professionals use terminology that may be unfamiliar outside their fields. CDC plain-language guidance recommends knowing the audience and purpose, choosing familiar words and numbers, and organizing information so that it is easier to understand and use.
That does not mean a localization team should independently simplify or replace approved medical meaning. It means the team should identify the audience before translation, use an approved terminology strategy, and send uncertain wording to a qualified reviewer. A professional training video for clinicians and a health education video for the general public may discuss the same subject, but they should not automatically use the same register.
Meaning may be split across audio and visuals
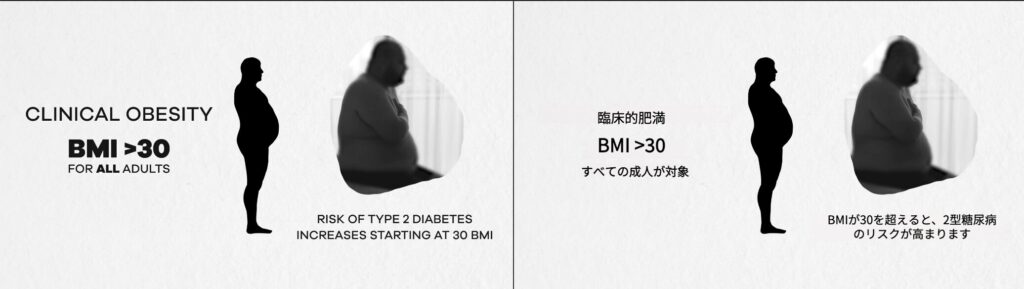
Consider a BMI explainer in which the narrator describes a category while the corresponding range appears in a chart. Or an anatomy video in which the narration refers to a location indicated by an arrow and label. The sentence may be translated correctly, yet the scene remains incomplete if the chart heading, range, or anatomical label stays in the source language.
Das ist der Grund visuelle Übersetzung belongs in the localization scope rather than being treated as a cosmetic finishing step. The visual layer may establish what a number represents, which body area is being discussed, or which step comes next.
A literal translation may still be hard to use
A literal translation can be grammatically correct without being suitable for the intended audience. Language variant, literacy, context, and familiarity with medical concepts can all affect how easily a viewer follows the material.
The Agency for Healthcare Research and Quality provides a practical review framework through its Patient Education Materials Assessment Tool for audiovisual materials, or PEMAT-A/V. It evaluates two separate qualities: understandability and actionability. Its criteria cover purpose, word choice, organization, visual aids, and whether the audience can identify what to do. These principles offer a useful review lens for multilingual patient education videos, even when an organization uses its own medical and linguistic approval process.
PEMAT-A/V does not assess medical accuracy. Clinical or subject-matter review remains a separate responsibility.
What Needs to Be Localized Beyond Subtitles?
Subtitles are only one layer of a patient education video. Before work begins, teams should review the entire asset and inventory every element that carries meaning.
- Narration and dialogue. Translate spoken explanations with the intended audience, approved terminology, and scene context in view. If dubbing is used, check whether the new pacing still aligns with the visual sequence.
- Subtitles and captions. Review terminology, line breaks, timing, and consistency with the spoken track. Captions may also contain speaker or sound information that ordinary subtitles do not.
- On-screen headings and labels. This includes anatomy labels, body areas, measurement categories, nutrition terms, chart legends, section titles, and callouts.
- Numbers and units. A number is not self-explanatory. Its heading, unit, category, decimal format, and surrounding instruction all affect how it is read. Any conversion or adaptation should follow the content owner’s approved policy rather than an automatic assumption.
- Steps and instructions. Numbered sequences, preparation steps, navigation prompts, and action labels must remain in the correct order and agree with the narration.
- Diagrams, tables, and interfaces. Arrows, legends, embedded screenshots, buttons, and fields can hold essential information even when they occupy only a small part of the frame.
This inventory helps teams decide which elements require medical review and which require visual or product review. An anatomy term may need a subject-matter specialist, while a translated app button may need confirmation from the digital-health product owner.
Which Videos Should Be Localized First?
The reviewed project samples point to several recurring types of visual health education: body measurements, nutrition and weight management, anatomy or body-location explanations, and structured health courses. These are sensible starting categories because their educational value often depends on visible text, diagrams, or organized steps.
A related sports science education case shows why slides, diagrams, formulas, and instructional text need to move into the target language with the spoken lesson.
Other organizations may also maintain patient-facing videos about procedure preparation, aftercare, medication use, medical devices, or digital-health tools. Those are adjacent industry applications, not patterns established by the reviewed sample. They should be prioritized only when they match the organization’s actual content library and audience needs.
Instead of choosing by topic alone, teams can rank candidate videos against six operational questions:
- Is there demonstrated demand for this language among the intended audience?
- How often is the video used or distributed?
- How much essential information appears inside the frame?
- Is the source video current and approved?
- Are the terminology and review owners known?
- Can the localized version be maintained when the source changes?
This approach avoids spending localization effort on an outdated asset simply because it is easy to translate. It also prevents teams from starting with a high-risk video before the necessary reviewers and terminology are available.
A Practical Workflow for Multilingual Patient Education Videos
1. Confirm the audience and approved source
Define who the video is for and where it will be used. “Spanish-speaking viewers” is not always a complete audience definition; region, communication setting, and expected health knowledge may influence terminology and tone. Confirm that the source video is the current approved version before extracting any text.
The source also needs a clear purpose. AHRQ’s audiovisual guidance asks whether the title, opening narration, or displayed text makes the material’s purpose evident. If the original video is ambiguous or overloaded, translation will reproduce that weakness rather than repair it.
2. Build a terminology sheet in context
Create a working glossary from approved scripts, existing patient education materials, product terminology, and previous translations. Include the source term, approved target term, definition or context, content owner, and any terms that must not be altered.
Do not collect only specialist nouns. Categories, action verbs, units, interface labels, and short warnings often create more consistency problems because they recur across voice, subtitles, graphics, and related materials.
3. Map the complete visual layer
Review the video scene by scene and record visible headings, labels, charts, annotations, captions, and interface text. Note when text appears, what object it refers to, and whether it is repeated elsewhere. This step catches information that a transcript-based workflow cannot see.
For the kinds of projects observed in recent usage, that can mean mapping a BMI table, diagram labels, terms inside a nutrition graphic, or headings embedded in a health course slide. Keep the visual inventory linked to the corresponding script segment so translators do not make decisions in isolation.
4. Translate connected elements together
Translate narration, captions, and visible text as parts of the same scene. When the narrator names a category shown in a chart, the spoken and visual terms should match. When an arrow points to a body location, the label should use the same approved terminology as the explanation.
This is also the stage to flag Texterweiterung. A target-language label may no longer fit inside a diagram or remain readable for long enough. Shortening it without review can change meaning, so linguistic and visual decisions need to be coordinated.
5. Rebuild the visual layer for the target language
Replacing text inside a frame is a design task as well as a translation task. The new wording must fit the available area, remain legible, and preserve its relationship with the diagram, table, body region, or action it describes. Font support, line breaks, contrast, placement, and display duration all need checking.
If the original design cannot hold a clear translation, revise the layout or shorten the wording with subject-matter approval. Shrinking text until it technically fits is not a useful solution when the audience can no longer read it.
6. Separate linguistic, subject-matter, and visual review
One reviewer rarely covers every risk. A language reviewer checks fluency, consistency, and audience fit. A qualified subject-matter reviewer checks whether the approved medical meaning, sequence, and terminology have been preserved. Visual QA checks placement, legibility, timing, truncation, and whether text still points to the correct object.
Review the finished scene, not only a spreadsheet of translated strings. Context can expose errors that look acceptable in isolation: a label attached to the wrong side of a diagram, a chart category that no longer matches the narration, or a line break that separates a number from its unit.
7. Evaluate the complete localized material
After corrections, watch the localized video from beginning to end. Check whether its purpose is clear, key information is organized, visuals reinforce rather than distract from the message, and any intended action remains identifiable. PEMAT-A/V can inform this review, but it does not replace an organization’s clinical, legal, accessibility, or language-access requirements.
Where appropriate, involve representatives of the intended audience. Internal reviewers can confirm terminology and policy; audience testing can reveal whether people understand the message as intended. The review method should match the video’s purpose and the organization’s governance process.
8. Maintain a version trail
Store the source version, target language, glossary, reviewer decisions, and publication date together. If the source changes, teams need to know which localized assets are affected. Version control is especially important when the same chart, label set, or explanation appears in several videos.
Common Localization Failures to Catch Before Publishing
The most visible failure is a translated voice playing over untranslated graphics, but it is not the only one. Teams should also watch for inconsistent terminology between narration and labels, specialist wording carried into public-facing content without review, translated text that covers an arrow or data point, numbers separated from their units, steps that appear in a different order from the narration, and outdated source information reproduced across several languages.
Automation creates another review trap: smooth wording can look finished before its meaning has been approved. AI can accelerate detection, translation, and rebuilding work, but it should not be treated as the medical reviewer or final authority. Healthcare content still requires the review process appropriate to its audience, subject, and organization.
Where Visual Translation Fits in the Workflow
Traditional video translation workflows often begin with the transcript, then produce subtitles or a dubbed track. That works for spoken content, but it does not automatically address text embedded in charts, slides, labels, annotations, or screenshots.
Vozo Visual Translate is designed for that missing layer. It detects on-screen text, removes the original text, translates it in context, and rebuilds the visual layer in the target language without requiring the original project file. Teams can compare source and translated text, edit or retranslate individual elements, adjust styling and layout, and refine animation timing before export. These controls are useful when a health education video contains compact labels, diagrams, course slides, or other text that must remain readable and consistent with the approved translation.
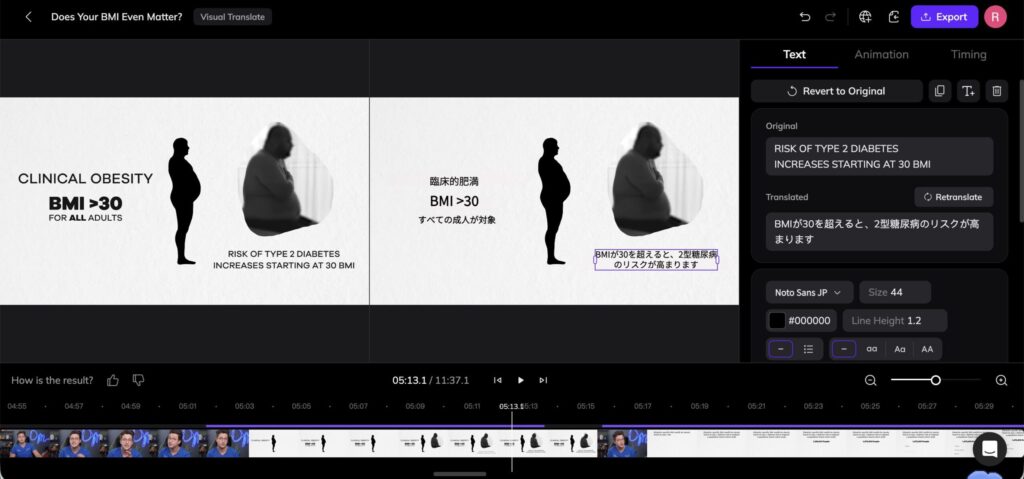
Visual Translate does not replace medical, linguistic, accessibility, or policy review. Its role is narrower and practical: it helps localization teams work on visible text as editable content instead of leaving it untranslated or manually rebuilding every frame. A complete video translation workflow can then add subtitles, dubbing, and lip sync.
A Final Review Checklist
Before publishing a localized patient education video, confirm that:
- The target audience, language variant, and source version are documented.
- Narration, subtitles, labels, diagrams, numbers, units, and instructions have all been inventoried.
- Spoken and visible terminology agree within each scene.
- No important source-language text remains on screen unintentionally.
- Translated text is readable and does not obscure the visual it explains.
- Medical meaning and intended actions have been reviewed by the appropriate owners.
- The finished video has been watched in context, not approved from text files alone.
- Review decisions and version information have been retained for future updates.
Build Multilingual Health Education Without Leaving the Visual Layer Behind
Patient education videos are easiest to localize when teams stop treating them as transcripts with pictures attached. Narration explains, but charts classify, labels identify, arrows direct attention, and on-screen steps organize action. All of those layers contribute to the message.
For healthcare educators and health-content teams working from an approved source video, the practical path is clear: define the audience, map every information layer, translate connected elements together, and keep qualified review in the loop. Visual translation can handle the on-screen text layer so diagrams, labels, headings, and instructions move into the target language alongside the rest of the video.
If your existing health education videos depend on visible text, review that layer alongside subtitles and dubbing before producing the next language version. The localization plan should begin with everything the viewer must hear, read, and follow.
Häufig gestellte Fragen
What is the difference between patient education video translation and localization?
Translation converts content from one language into another. Localization adapts the complete video for a target audience and may include narration, subtitles, on-screen text, terminology, layout, timing, units, and review. In a visual health education video, localization also checks whether spoken and displayed information still agree.
Are translated subtitles enough for a patient education video?
Not when essential information appears inside the frame. Anatomy labels, chart headings, measurement categories, steps, warnings, or interface text may remain inaccessible if only subtitles are translated. Teams should inventory the whole video before deciding which layers require localization.
How should medical terminology be handled across languages?
Start with approved source materials and a terminology sheet. Match the language to the intended audience without independently changing the approved meaning, then have uncertain or consequential wording reviewed by qualified language and subject-matter reviewers.
Can AI translate patient education videos without human review?
AI can support transcription, translation, dubbing, and visual text processing, but it should not replace the review required for healthcare content. The appropriate reviewers depend on the video’s audience, subject, intended use, and the organization’s governance requirements.
What types of visual text can be localized in a health education video?
Common examples include headings, anatomy labels, body-area callouts, chart legends, measurement categories, nutrition graphics, numbered steps, annotations, and interface text. The exact scope should be established through a scene-by-scene visual inventory.
How can teams assess whether a localized video is understandable?
Teams can combine their internal review process with established health-literacy criteria. AHRQ’s PEMAT-A/V evaluates whether audiovisual patient education materials are understandable and actionable, including their purpose, organization, language, visual aids, and presentation of actions. It does not assess medical accuracy.